
Therapeutic Relationship and Cognitive Interweaves in EMDR Therapy
Guest Blog Post by Aurora Luna Walss, LMFT
What does a therapist do when a client is looping in EMDR therapy reprocessing, or when a client appears stuck and reprocessing is blocked? Perhaps a short answer to these questions is that the therapist needs a mindful attitude and to select appropriate interventions or interweaves, especially when working with complex trauma. However, what if a safe and comprehensive therapeutic relationship within the framework of the Adaptive Information Processing (AIP) model is actually the most important factor in answering these questions?
Building a safe therapeutic alliance
Within the framework of EMDR therapy, the therapeutic relationship develops and evolves to help the client more effectively regulate emotions, develop resources, explore and reprocess traumas, and build a present and future vision in which they see themselves as healthy and fulfilled. Emotional attunement and rapport building between the therapist and the client in the initial stages of therapy emphasize the importance of this secure relationship in which the healing of trauma might occur.
Hase and Brisch (2022), describe EMDR as a sensitive psychotherapy. They also state that a description of the therapeutic relationship in EMDR therapy is necessary for the development of EMDR therapy as a psychotherapeutic approach. Hase and Brisch (2022) state:
In our opinion EMDR can be described as a “sensitive” psychotherapy approach. It could explain partly the specific therapeutic relationship in EMDR Therapy, which seems to develop rapidly and offer a safe environment, which allows our clients to reprocess, to grow and to get past the past (p 5).
The therapeutic relationship in EMDR therapy is a current and evolving matter of interest and research. In 2022, Hase and Brisch provided a description of the therapeutic relationship in EMDR therapy based on Bowlby’s attachment theory. In 2025, Hase et al. conducted a survey to test this definition, and included the sensitive behaviors a therapist should show in order to promote a positive EMDR experience for the client:
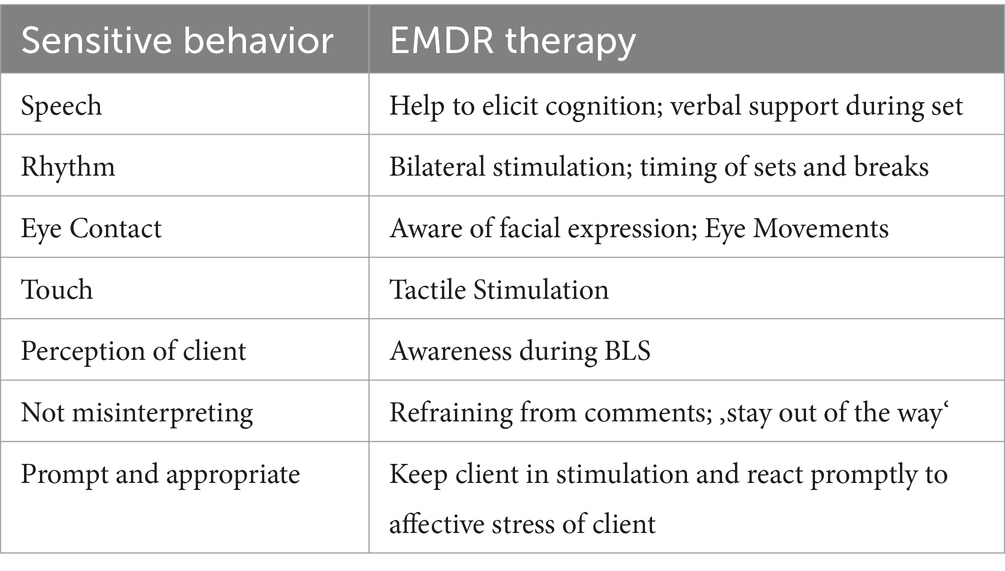
Hase et al., 2025 https://doi.org/10.3389/fpsyg.2025.1519665
The role of mindfulness
To develop these sensitive behaviors, the state of mindfulness, both for the therapist and the client, is fundamental in EMDR therapy. According to Daniel Siegel’s (2010) definition, mindfulness refers to the ability to keep full attention in the present moment, with an open attitude and without judgment toward internal or external experiences. This practice allows for greater awareness and connection with oneself and others. A present therapist develops a better understanding of the client and a deeper quality of observation of the body language, gestures, postures, and signals the client expresses, besides the symptoms described. A profound understanding of the clients’ needs will lead to a good enough understanding of them all throughout the therapeutic process.
The practice of mindfulness can be enhanced during the preparation phase of EMDR, in which emotional regulation is the vital component. This phase should be developed with the time and respect it deserves, understanding that the client’s safety is paramount and that the therapist’s personality, tone of voice, language, body language, and willingness to pace themselves. This preparation informs the interventions and cognitive interweaves the therapist may use in reprocessing phases and during closing procedures. In Hase’s (2021) article The structure of EMDR therapy: A guide for the therapist, Hase cites Dr. Francine Shapiro in highlighting the importance of the preparation phase in EMDR, which provides the client with the necessary resources before the subsequent phases. Hase emphasizes how mindfulness helps the therapist remain present and receptive, fostering a more effective and sensitive intervention that allows the client to experience safety, while the therapist achieves a gradual approach based on attunement and connection with the client.
In addition, in her book Polyvagal-Informed EMDR, Rebecca Kase highlights the importance of respecting the rhythm of the client’s nervous system. Kase argues that integrating polyvagal theory allows the therapist to better understand and work with defense responses and self-regulation capacities.
In this way, each intervention conducted in the initial phases of EMDR therapy makes the alliance stronger and more secure. It also promotes attunement, connection, and resonance, facilitating the subsequent selection of specific cognitive interweaves and/or interventions appropriate for each client during treatment.
Cognitive Interweaves
Cognitive interweaves, a concept developed by Dr. Shapiro, are brief clinical interventions used during the reprocessing phases of EMDR that help clients restructure negative cognitions and blocking beliefs. These interweaves allow clients to challenge and modify limiting beliefs, promoting the integration of new perspectives and adaptive solutions.
In the fourth phase of EMDR therapy, dedicated to desensitization and reprocessing, cognitive interweaves play a crucial role in the repair of developmental trauma. This type of trauma, which often originates from adverse childhood experiences, requires a careful and gradual approach.
Using cognitive interweaves allows clients to address and modify the limiting beliefs that sustain the trauma state, assisting the integration of experiences and the resolution of internal conflicts. Through Socratic questioning, the therapist can gently challenge the client’s negative beliefs that emerged during development. Metaphors and reframing help recontextualize and reinterpret traumatic experiences, promoting adaptation and resilience.
The incorporation of polyvagal theory into cognitive interweaves focuses on the regulation of the autonomic nervous system. This theory, proposed by Stephen Porges, provides a framework for understanding how physiological responses can be modulated during the reprocessing of traumatic memories.
Dr. Shapiro created these interweaves primarily to work with clients with complex trauma (Shapiro, 2001, p. 258); however, she realized that any client could experience blockages or circumstances that require these interventions and proposed four scenarios where cognitive interweaves could be used when spontaneous processing seemed to be insufficient for therapeutic objectives:
- when looping occurs
- when information is insufficient to process
- when presented with a lack of generalization
- when time pressure exists during the session.
Interweaves are used to obtain adaptive material stored, to add needed education, to connect adaptive memories, to help disconnect from maladaptive memories, or to broaden the client’s perspective. Good timing and sequence are important for interweaves to be successful. It is important for the therapist to understand a client’s unique cognitive and emotional plateaus, and their unique negative cognitions and beliefs, so as to better assist when accompanying a client on the journey of reprocessing toward positive resolution.
Clinical Interweaves Categories (CIC) developed by Laliotis & Korn (Hensley, 2015) follow the acronym EMDDRIIAA as follows: Experiential, Modulation, Defense, Development Repair, Relational, Informational, Integrating, Action, Access. Korn and Baldwin (2021) have highlighted the importance of emotional regulation and guided mindfulness in the repair of developmental trauma. This type of cognitive interweave allows the client to keep a state of calm and mindfulness, helping the integration of painful memories and the construction of new narratives. Although objective observation and decision making to “stay out of the way” from the therapist are fundamental for the EMDR process, the appropriate selection of cognitive interweaves is crucial for progress in EMDR therapy.
Clients need presence, attunement, and connection with the therapist to address their trauma. Each implies attention, concentration, a strong connection, as well as precise and objective physical and verbal interactions within the virtual therapeutic alliance. The therapist´s sensitivity, support, and embodied connection are perhaps the most important tools for the therapy to be successful. In this regard, additional scientific research about the therapeutic relationship in EMDR, and its influence throughout each phase, is needed (Hase et al., 2025). This presents a wonderful and interesting world of opportunities for those curious professionals to advance research in this field.

Aurora Luna Walss is a Licensed Marriage and Family Therapist with over a decade of experience in private practice helping adults navigate trauma. EMDR is her primary therapeutic approach although she incorporates Internal Family Systems, Expressive Arts Therapy and Mindfulness. Luna Walss is an EMDRIA Approved Consultant™ and offers a variety of advanced courses in EMDR therapy.
References
Hase, M. (2017). EMDR as a therapy for PTSD: Trauma processing and stabilization. Springer.
Hase, M. (2021). The structure of EMDR therapy: A guide for the therapist. Frontiers in Psychology, 12, 660753. https://doi.org/10.3389/fpsyg.2021.660753
Hase, M., & Brisch, K. H. (2022). The therapeutic relationship in EMDR therapy. Frontiers in Psychology, 13, 835470. https://doi.org/10.3389/fpsyg.2022.835470
Hase, M., Brisch, K. H., Solomon, R. M., & Hase, A. (2025). The therapeutic relationship in EMDR therapy – A survey. Frontiers in Psychology, 16, 1519665. https://doi.org/10.3389/fpsyg.2025.1519665
Hensley, B.,(2015). An EMDR therapy primer, second edition: From practicum to practice. Springer Publishing Company.
Kase, R. (2023). Polyvagal-informed EMDR: A neuro-informed approach to healing. Norton and Company.
Korn, D. L. & Leeds, A. M. (2002). Preliminary evidence of efficacy for EMDR resource development and installation in the stabilization phase of treatment of complex post-traumatic stress disorder. Journal of Clinical Psychology, 58(12), 1465-1487. https://doi.org/10.1002/jclp.10099
Korn, D. L., & Baldwin, M. (2021). Every memory deserves respect: EMDR, the proven trauma therapy with the power to heal. Workman Publishing.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Shapiro, F. (2001). Eye movement desensitization and reprocessing (EMDR): Basic principles, protocols, and procedures. Guilford Press.
Siegel, D. (2010). The mindful therapist: a clinician’s guide to mindsight and neural integration. W. W. Norton & Company.
Back to Focal Point Blog Homepage
Additional Resources
If you are a therapist interested in the EMDR training:
- Learn more about EMDR therapy at the EMDRIA Library
- Learn more about EMDR Training
- Search for an EMDR Training Provider
- Check out our EMDR Training FAQ
If you are EMDR trained:
- Check out the EMDRIA Let’s Talk EMDR Podcast
- Check out the EMDRIA Focal Point Blog
- Learn more about EMDRIA membership
- Search for EMDR Continuing Education opportunities
If you are an EMDRIA™ Member:
- Learn more about EMDR Consultation
- Find clinical practice articles in the EMDRIA Go With That Magazine®
- Search for articles in Journal of EMDR Practice and Research in the EMDRIA Library
Related Articles



